

Pituitary Tumours
The Pituitary Gland
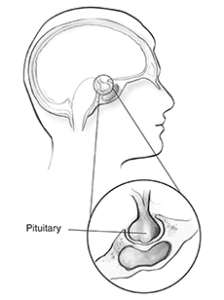 This is a small gland which measures the size of two peas. It sits in a bony depression at the base of the skull. This gland is attached by a stalk to an area of the brain called the hypothalamus. The pituitary works as a master gland, releasing chemicals that regulate other glands around the body. It works to balance hormones which are essential for normal life.
This is a small gland which measures the size of two peas. It sits in a bony depression at the base of the skull. This gland is attached by a stalk to an area of the brain called the hypothalamus. The pituitary works as a master gland, releasing chemicals that regulate other glands around the body. It works to balance hormones which are essential for normal life.
The pituitary gland is thought as having two halves, anterior and posterior. Important hormones which it secretes include:
Anterior Pituitary
ACTH: Acts to stimulate the release of cortisol from the adrenal glands. Cortisol is important for metabolism, regulating sugars and the immune system.
TSH: Works on the thyroid gland to stimulate the release of thyroid hormone (T3 and T4). Thyroid hormone is important in energy utilisation and temperature tolerance.
GH (Growth Hormone): Encourages the release of IGF-1 from the liver. IGF-1 is important in growth before puberty and may have some role in the maintenance of soft tissues in adulthood.
FSH/LH: Act on the ovaries / testicles for the production of sex hormones. These include oestrogen and testosterone.
Prolactin: Involved in breast milk secretion.
Posterior Pituitary
Antidiuretic Hormone (ADH): Essential for water reabsorption in the kidneys and maintaining fluid balance. Influences the concentration of sodium (salt) in the body.

Pituitary Tumours
These are usually slow growing and benign (non-cancerous) tumours. They rarely spread around the body but can invade into the structures around the pituitary fossa. Tumours are either ‘functioning’ or ‘non-functioning’.

Grey areas are vision loss
Functioning tumours
These produce a hormone excess dependent on the cell type from which the tumour grows. They produce their effects by releasing an excess of one or two pituitary hormones. Hormone excess may lead to conditions like:
- Cushing’s disease (ACTH excess)
- Acromegaly / Gigantism (GH excess)
- Hyperprolactinaemia (Prolactin excess)
- Hyperthyroidism (T3/T4 excess)
Non Functioning tumours
These are the most common. They cause their symptoms by upwards expansion compressing important structures. This can lead to:
- Visual loss. Especially the outer visual field for each eye. Classical visual field loss is shown in this picture.
- The Inadequate production of pituitary hormones needed for normal body functions. Hormone levels can be measured with blood tests and replaced with oral tablets (and nasal spray) if necessary.
Common tests
- Blood tests, including studies of hormones levels.
- Eye specialist reviews including visual field tests.
- MRI scans to measure how big the tumour is and where it is located. This helps to guide the surgery and watch for regrowth after an operation.
Treatment
Functioning Tumours
The goal of surgery is to remove your tumour and bring the hormone levels down. Total cure is when your hormone levels return to normal and the tumour does not recur. Unfortunately in some cases this is not possible. Surgery can often help reduce the levels of hormone to more manageable levels. Additional surgery or therapy such as injections of hormone inhibitors or radiotherapy might be necessary.
Non-Functioning Tumours
Surgery is required when a visual disturbance is noted to protect sight in the long term. Often these tumours can be found incidentally by tests performed for other medical reasons. Removing these tumours can be important to keep the normal pituitary healthy. Occasionally they may grow into the canvas like covering (dura) and venous channels (cavernous sinuses) around the pituitary fossa. This can make total removal very difficult.
Endoscopic Trans-sphenoidal Surgery
 Surgery on the pituitary is now generally carried out through the nose. At the back of the nose is an air filled cavity called the sphenoid sinus. This lies directly underneath the pituitary fossa which contains the pituitary gland.
Surgery on the pituitary is now generally carried out through the nose. At the back of the nose is an air filled cavity called the sphenoid sinus. This lies directly underneath the pituitary fossa which contains the pituitary gland.
During the operation, surgeons are assisted by image guidance to give precision. This guidance requires a CT scan before the operation.
Surgery is performed using an endoscope. This is a telescope containing fibres for light and a lens for vision. The high quality camera shows the images on a TV screen. This enables a clear view of structures during the operation. Both nostrils are used for the passage of instruments and the endoscope.
There are two components to the surgery:
- Access through the nose to the sphenoid sinus. There are natural drainage holes that connect the nose to the sphenoid sinus. These are identified and enlarged to enable access to the pituitary fossa and the second part of the operation. Often specialist Ear, Nose and Throat surgeons help with this.
- Removal of the tumour. The tumour is then removed with a series of ring shaped curettes and suction. Often it comes out in a series of small fragments. In smaller tumours (microadenomas <1cm), it is often possible to separate the tumour from the remaining gland. In larger tumours (macroadenomas >1cm), the remaining gland is reduced to a sliver of residual tissue.
If the gland is functioning normally, a proportion of patients will be left with sufficient residual pituitary gland that functions normally. Otherwise, patients might need to take hormonal replacement long term. If the gland is not functioning preoperatively, it is unlikely that the surgery will allow recovery of the residual gland’s functioning.
The roof of the pituitary fossa is a very thin “gladwrap” like membrane called the diaphragma sella. This membrane separates the pituitary gland from the pool of cerebrospinal fluid (CSF) that surrounds the brain. A small hole in this membrane might lead to a leak of CSF through the nose. CSF leakage increases the risk of infection around the brain (meningitis). Perforations can occur when a tumour previously abutting the membrane is removed. To seal this, collagen grafts are used. Occasionally fat is taken from around the belly button to reinforce the graft. Achieving a watertight seal can be very difficult and some patients need to return to the operating room.



Risks and possible complications of surgery
Surgery around the pituitary gland carries its own special kinds of risks. Risks can include: Death, stroke, bleeding, cerebrospinal fluid leak (and subsequent need for a fat graft), infection, headaches and visual decline. Some patients will require further surgery, hormonal supplements or other specialist therapy. The most serious risk relates to an injury of the carotid arteries on either side of the gland.
Medications
Most tumours require surgery to remove their bulk and take pressure off the surrounding structures. The exception to this are prolactinomas. These tumours are often effectively managed with medications such as bromocriptine or cabergoline.
In functioning tumours, the goal is to provide a biochemical cure. Sometimes this means further medications, surgery or radiotherapy will be required.
After surgery, specialist endocrinologists are essential to monitor progress. This is because approximately a third of patients will need hormone replacement. Tablets could include hydrocortisone, thyroxine, testosterone, GH or oestrogen. Occasionally a nasal spray containing ADH is used. Your endocrinologist will work out your ongoing medication requirements after surgery.
MRI Pituitary pre and post-surgery

Postoperative Management
Most people come in the day of or night before surgery. The night after surgery is spent in the High Dependency Unit (HDU). Here the patient’s blood pressure and fluid balance are monitored. Checks are made for nose bleeding. It is not a terribly painful operation, however adequate pain relief is always available. When stepping down from the HDU, patients will continue to be closely watched. For the duration of your hospital stay everything you drink and urinate will be measured. This will be aided by the use of a urinary catheter inserted in the operating room.
On discharge, medication requirements will be discussed with you. The most common requirements are hydrocortisone (to replace Cortisol) and Minrin (to replace ADH). Any medications started prior to surgery will need to be continued. Changes in medication will then be recommended by your endocrinologist.
A follow-up appointment with your endocrinologist should be made at 4-6 weeks, with your neurosurgeon 6-8 weeks and your eye specialist (if you had visual problems preoperatively) at 3-6 weeks postoperatively.
Heading home
- All patients will get nose and forehead pain. This is managed with celecoxib and paracetamol as prescribed by your doctor.
- Every patient must do nasal washouts. This should start 5 days after discharge and continue twice daily for 10 weeks. “Neil’s Sinus Rinse” is available from pharmacies.
- Patients must be active in the days after surgery. Activity is important for recovery and helps prevent deep vein thrombosis (DVT). This is when blood clots form in veins, primarily of the legs. You should resume normal activities at home and walk twice daily. Do not overexert yourself. This means no straining for 6-weeks (including at the gym or on the toilet!). Laxatives and a high fibre diet can help with constipation.
- All patients should restrict their fluid intake. Patients may only consume 1 to 1.2L of fluid per day for 3 to 4 weeks postoperatively. This includes water, coffee, tea, soups etc. See below for more information.
- Take hydrocortisone medication as prescribed. See below for more information.
- You are allowed to drive after trans-sphenoidal surgery as soon as you are feeling well. However, if you had a preoperative visual problem or notice any worsening in your sight after surgery, you will need to have your optician confirm that your visual fields have expanded enough to satisfy Land Transport Safety Agency (LTSA) regulations.
- If a fat graft was taken, the sutures used to close the wound at the belly button are dissolvable and do not need to be removed. This area needs to be kept clean and dry. Redness, discharge or signs of infection need to be reported to your GP.
If you become unwell after surgery, you need to report promptly to your general practitioner (GP)
The usual causes of problems postoperatively include:
- Low salt (sodium) in the blood
Often caused by a condition called SIADH. This is when too much of the hormone ADH is released. ADH stimulates the kidneys to reabsorb water. Too much water absorption can decrease the body’s concentration of sodium. If severe enough, this can make you very sick with nausea, vomiting and seizures. Pituitary surgery makes you particularly susceptible to this and it is common in the first 2 to 3 weeks after the operation. To help prevent this, all patients should restrict their fluid intake to 1 to 1.2L for 3 to 4 weeks postop. This includes all fluids e.g. coffee, tea, soups etc.
The only exception is if you develop another condition called diabetes insipidus (DI). This is pituitary diabetes and not sugar diabetes (diabetes mellitus). This condition will be discussed with you separately if necessary. DI is characterised by high volumes of clear urine, increased thirst and needing to urinate frequently (including at night). If this happens, drink to thirst and contact your GP or endocrinologist.
- Inadequate cortisol replacement
This can lead to similar symptoms to SIADH. You must make sure you are taking your hydrocortisone medication. Your GP or endocrinologist can adjust the dose if you are not getting enough. Your endocrinologist will test you to find out if you need to continue the hydrocortisone. If you are physically unwell for any reason, DOUBLE the dose of hydrocortisone for 2-3 days and discuss further with your doctor.
- Infection
These occur infrequently and can range in severity and location. Meningitis may require a hospital stay for antibiotics. Sinusitis can be managed at home with nasal decongestants and oral antibiotics. Patients who get sinus symptoms should visit their GP.
- Nose bleeding
Occasionally after surgery patients can suffer nose bleeding. This is especially if you over exert yourself. The first step is to sit down and try and relax. Most bleeding stops in a few minutes. If it continues and is profuse, get to your local medical centre and they will consider placing nasal packs to control the bleeding.
- Cerebrospinal fluid (CSF) leak
A profuse leak of watery fluid from the nose, especially when you tip your head forward can signal a leak of CSF. This fluid might taste very salty. If it continues more than once, you need to contact your GP or Neurosurgeon. Some patients need a trip back to the operating room.
Months to years after surgery
Around 15-30% of non-functioning tumour patients will need additional therapy. This could be in the form of repeat surgery or radiotherapy at some stage in their 10 year follow-up. Redo surgery tends to be similar to the initial surgery and does not carry any significant additional risk.
Ongoing Follow-up
Patients with functioning tumours will be reviewed by their endocrinologist. Tests will be performed to determine whether they are cured or need additional treatment.
Patients with non-functioning tumours will be reviewed by their neurosurgeon for a postoperative check around 2-3 months postoperatively. Postoperative MRI scans will be arranged for you. Often these continue for 10 years postoperatively. Regular review by your endocrinologist is essential.
Surgical Photos
Here are some photos of the surgery looking down the microscope. Although it may appear bloody these photos are magnified a great amount. Remember the pituitary gland is around the size of two peas!

- Dura B. Opening dura C/D. Tumour E. After tumour removal F. Roof G. Patch H. Glue I. Flap

Consent
Surgery is a serious event that carries risk. It is imperative that patients are understanding and familiar with these risks before undergoing an operation. Before your surgery, you must be familiar with the goals, outcomes and possible complications for the procedure. Utmost care is always taken to minimise undesired outcomes. Patients must discuss their treatment with the surgeon before the operation.